Retake
P13) Worsening hip pain in a 5-year-old
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a pediatric patient with difficulty ambulating.
- Review the DDx considerations in a pediatric patient with difficulty ambulating.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a pediatric patient with difficulty ambulating.
History
A 5-year-old child presents with a 6-week history of worsening right hip pain and limping, without any history of trauma. The pain is exacerbated by activity. The patient spent the last two months in the Ozark mountains of Arkansas, but has no recent history of fever, rash, or respiratory illness. The patient's vaccinations are up to date.
Physical Exam
BP: 105/70, HR 80, RR 28, Temp 98, O2 saturation 99%.
MSK: Antalgic gait favoring the left leg, and restricted movement on passive and active range of motion of the left hip.
Labs
The WBC count is within normal limits.
Provisional Diagnosis
Select the Dx you believe is most appropriate
Based on the clinical presentation, Legg-Calvé-Perthes disease is the most likely diagnosis. It is avascular necrosis of idiopathic origin that most commonly presents in males aged 5-8 years. The condition is characterized by insidious onset of hip pain that is exacerbated by activity and commonly manifests as a limp. The normal WBC count and lack of fever make a septic joint less likely. DDH is more commonly present in younger infants and may present with a hip click, positive Ortolani/Barlow maneuver, or a limp. SCFE typically affects patients between 11-15 years old with obesity or endocrine disorders.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
This patient requires routine, but expedited workup.
First Imaging Study
What is the first imaging study you will order?
A radiograph of the right hip would be the best first line, readily available, low-cost imaging modality. It can show bony changes associated with LCPD.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
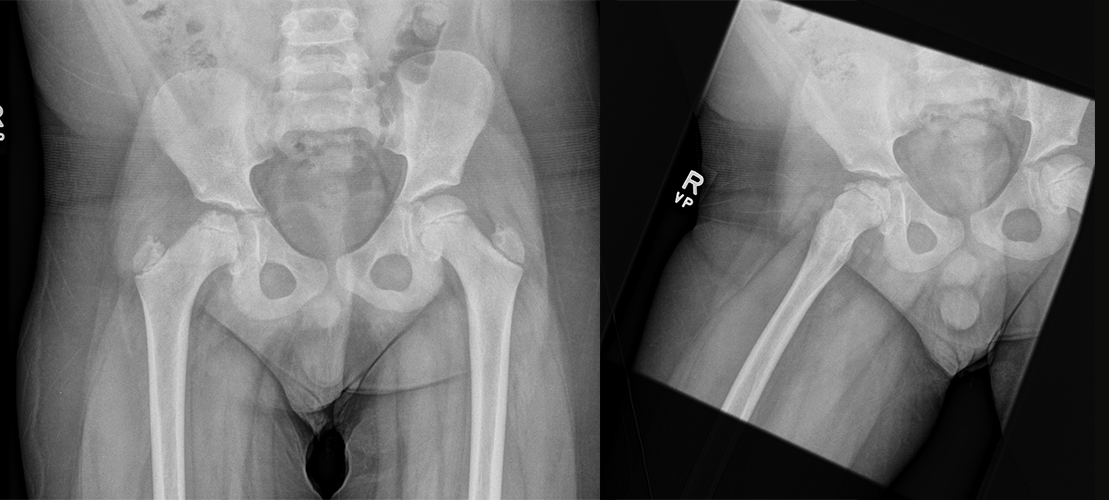
Hip XR
What is the imaging finding in the right femoral head?
Osteonecrosis is the visualized imaging finding considering the flattening of the femoral head, which is consistent with LCPD. Osteoporosis is a generalized decrease in bone density throughout the skeleton, while osteomyelitis is a bacterial infection characterized by increased bone density and inflammatory changes like reactive sclerosis, bony destruction, and edema.
Is there a difference in size between the right and left femoral heads?
There is a reduction in the size of the right femoral head relative to the left. This is another characteristic of osteonecrosis in LCPD.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
No further imaging is indicated.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
The patient’s presentation and imaging are highly suggestive of Legg-Calvé-Perthes disease.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient requires routine, but expedited workup.
Assessment and Plan
Please provide your assessment and plan for this patient
The patient is a 5-year-old male presenting with clinical and imaging findings indicative of right-sided Legg-Calvé-Perthes disease (LCPD). A referral to a pediatric orthopedic specialist should be made for a comprehensive evaluation and management plan, which may encompass surgical osteotomy or conservative treatment options. Analgesics should be administered, and the child should avoid weight-bearing on the right side until assessed by the specialist.
Lessons Learned:
- Legg-Calvé-Perthes disease (LCPD) arises from avascular necrosis of the femoral head without any prior traumatic event.
- The pathophysiology and the underlying mechanisms causing blood supply disruption, which lead to avascular necrosis, remain unclear.
- LCPD can manifest unilaterally or bilaterally and typically affects children between the ages of 5 and 8.
- Although MRI is the preferred imaging method for detecting early-stage LCPD, X-rays can reveal characteristic features, especially in advanced cases.
- Treatment strategies depend on the severity of the condition.
- In milder cases, reduced weight-bearing and physical therapy are often recommended, while surgical intervention may be necessary in more severe instances.
- The age at onset and the extent of femoral head involvement are crucial prognostic factors.
- While most children recover from LCPD, some may experience long-term complications such as arthritis or discrepancies in leg length.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}